Co-Authored with: 1@prosper , 1@omielp, 2Mabel Nakawoya, 2Arinaitwe Moses, 2Vincent Kamara, Pauline Amuge, 2Ebony Quinto, Adeodata R. Kekitiinwa, 2Stavia Turyahabwe
Institutions:
- Health Information Systems Program- Uganda,
- National TB and Leprosy Program, Ministry of Health, Uganda
- Baylor College of Medicine Children’s Foundation–Uganda
Summary
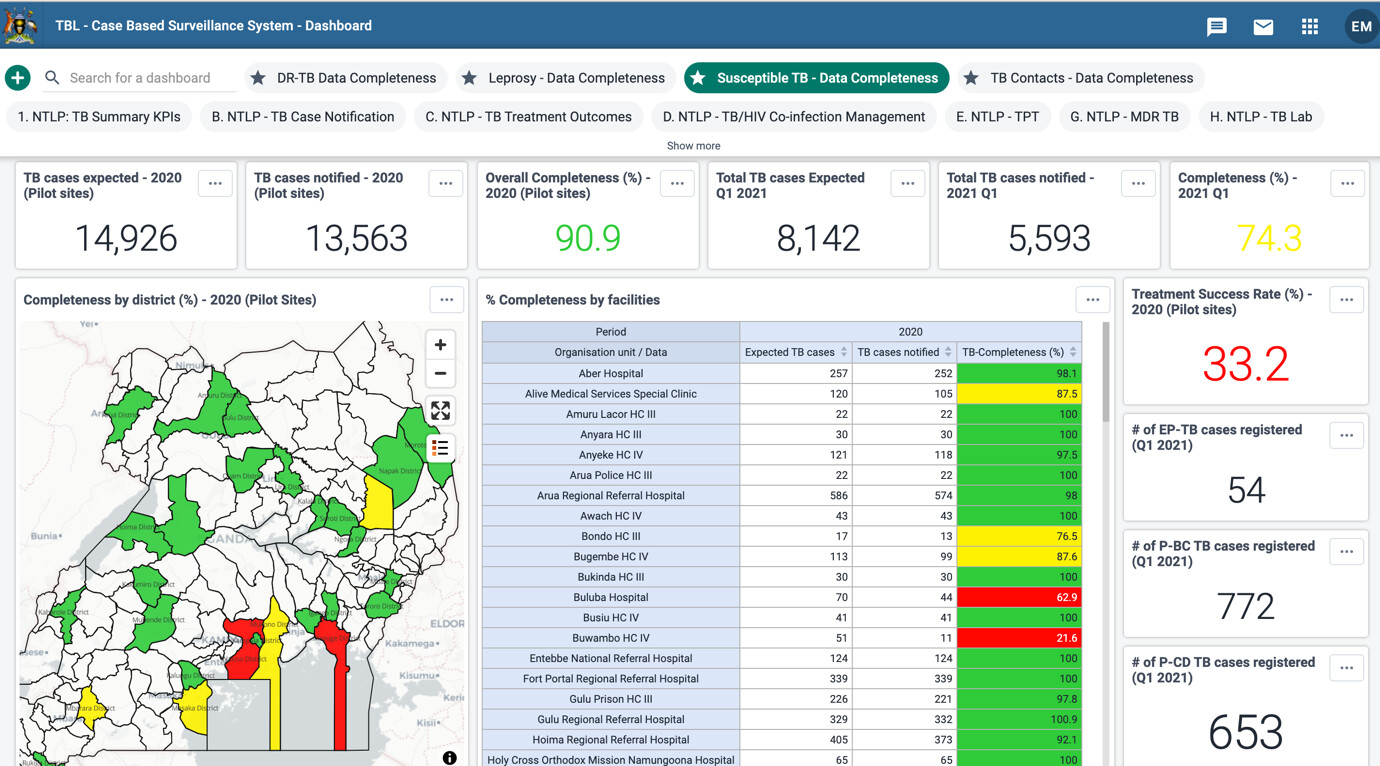
The National TB and Leprosy Program in Uganda started piloting the TB and Leprosy case-based surveillance system in 97 health facilities in 2021; 86% (83/97) has started data entry with 58% (8,122/14,589) of expected records captured. Uptake of the system has been influenced by a dedicated technical eCBSS working group, feedback meetings, sufficiency of internet bundles, availability of human resources, presence of computers and network.
Background
Uganda Ministry of Health has previously relied on aggregate data for TB reporting and decision making whose generation is cumbersome and prone to errors. Aggregate data limits access to patient-level data for monitoring and operational research. The National TB and Leprosy Program (NTLP) developed an electronic TB case-based surveillance system (eCBSS), with stakeholder involvement and CDC funding. We demonstrate the uptake of the system after 7 months of piloting, 9 months of scale-up, and the key influencing factors.
Intervention
Using the World Health Organization (WHO) health data toolkit for planning information systems, we gathered end-user requirements. These informed the eCBSS development to manage data for notification and follow up of patients with drug-susceptible TB, drug-resistant TB and leprosy m The system was initially tested in 7 urban and peri-urban sites. This was followed by national and regional trainings reaching 515 participants, piloting of the system in 97 facilities and scaling up to 228 facilities across Uganda. Follow up technical assistance continued through support supervision visits, provision of data bundles, monthly updates meetings and user support on online platforms. We conducted an evaluation that included in-depth interviews to assess the implementation
Results
After 7 months of piloting and 9 months of scale up, 83 (86%) pilot facilities had started data entry with 58% (8,122/14,589) of expected TB case notification records captured. Enabling factors mentioned by interviewed health workers in facilities with over 90% of records captured included; weekly feedback meetings: 52% (50/97), sufficient internet bundles: 52% (50/97) and availability of computers / laptops: 52% (50/97). Health facilities that had not yet entered up to a half of their expected records expressed challenges of insufficient human resources: 13% (13/97), insufficient laptops: 13% (13/97), limited internet access: 11% (11/97) and poor network connection: 10% (10/97).

Uptake of electronic TB case-based surveillance and reporting is feasible and can be achieved through intensive weekly site support and feedback meetings, sufficiency of internet access, availability of human resources, presence of computers as well as network.