1. Background of Tanzania Electronic Immunization Systems
To successfully reach children with life-saving vaccines, vaccine supply chains must achieve the six “rights”, as identified by WHO: right product, right quantity, right condition, right place, right time and right cost . Achieving each of those ‘rights’ requires the use of quality information by data managers at each level i.e national, sub-national and at health facility level.
The Tanzania’s Ministry of Health (MoH) through its Expanded Program for Immunization (EPI) program implemented the Electronic Immunization Registry (TImR) in 2016 to support the management of vaccine and logistic information at the health facility. Prior to launching TImR, the immunization information was digitalized down to the district level, and paper-based at health facility level. District managers received monthly paper reports from health facilities and submitted monthly reports into the Health Management Information System (HMIS) based platform using District Health Information Software 2 (DHIS2), and the Vaccine Information Management System (VIMS). At the facility level, the healthcare workers use TImR to register children receiving vaccinations, document vaccines administered and identify children who are off schedule. The TImR web-based portal generated routine aggregate reports for sharing with data managers at district level and above.
2. The challenge with parallel Information Systems
The adoption of parallel systems managing Immunization data (i.e TImR, VIMS and DHIS2) in Tanzania have led to undesired outcome or delays in achieving the intended objectives of introducing information systems. The parallel systems are not well streamlined and linked leading to data duplication and discrepancy among the systems managing Immunization data. For example, while some regions are using TImR at the facility level to manage immunisation data, the health workers are still required to fill in the HMIS registers for the Child Health and submit them at the district level for data entry in the DHIS2 and VIMS. This has led to duplication of reporting efforts resulting to overburdening already overstretched healthcare workers.
Furthermore, there is little to no collaboration among the departments managing the parallel systems leading to inconsistent of immunization information being reported and used at the national and sub-national levels. For example, the MoH uses DHIS2 platform as its health data repository and the means for communicating and disseminating health information to its stakeholders. However, there are inconsistency between the immunization information available within the DHIS2 and other immunization systems used by the EPI programme. This has led to confusion and uncertainty among stakeholders of the accessibility of appropriate and accurate immunization information.
To address, such challenge, the MoH with its partners such as HISP Tanzania, JSI and PATH embarked on a mission of integrating the Immunization Systems and improve the accessibility of quality immunization data within the national DHIS2 platform.
3. Systems interoperability for Improved Information Use.
The integration between the Electronic Immunization Systems (EIS) and DHIS2 provided a benchmark for strengthening immunization data management and information use at national and sub-national levels. The information interoperability addressed the challenges of systems fragmentation providing a common shared source of immunization information. This required an innovative way of approaching normally routine activities, and a rigorous system for monitoring the immunization programmes.
HISP Tanzania played a pivotal role in ensuring the systems interoperability between EIS and DHIS2 becomes a reality. Two regions (i.e Mwanza and Kilimanjaro region) were designated as ‘paperless’ regions and capacitated to report using TImR and remove manual reporting through the HMIS registers. TImR, was configured through its web-based portal to aggregate and send immunization data into DHIS2 and form part of the national health data repository. Similarly, TImR was configured to share vaccine and logistics information to VIMS for management purposes. VIMS, on the other hand, sends stock data to TImR for management and distribution of immunization stock at the health facility level.
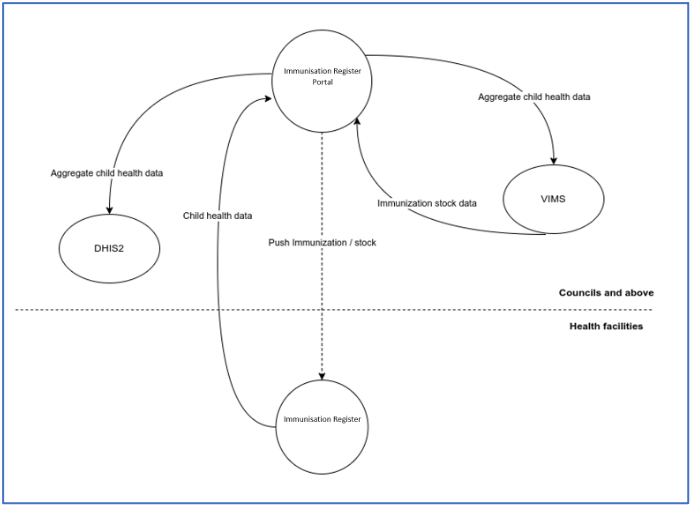
Figure 1: Integrated Systems Architecture between EIS with HMIS (DHIS2)
4. Results from Integrating EIS and DHIS2
The streamlining and linking between the EIS and DHIS2 has provided an avenue whereby data managers at national and sub-national levels can use consistent immunization data for decision making. The HMIS and EPI department can now use shared DHIS2 platform for analyzing and disseminating immunization information leading to making better plans and monitor performance based on the targets set. The consistent accessibility of Immunization data within the DHIS2 platform provides stakeholders with improved confidence of the shared information and strengthen the collaboration among participating actors.
In addition, the integration between the EIS and DHIS2 has eased the additional burden of redundancy data collection for healthcare workers. With the information interoperability, the DHIS2 has brought fragment immunization data systems into one platform. The integration has also reduced management costs in the ‘paperless’ regions in a way that limited available resources can be allocated into other areas of higher importance. For example, the printing costs for registers, tally and summary sheet for Child Health have been reduced significantly within the paperless regions as the digital systems are used for capturing and managing immunization data.
Having a single source for data use and analysis has increased the numbers of users especially Regional immunization officers (RIVO) and District Immunization Officers (DIVO) to use immunization data using DHIS2 to monitor and strengthen service delivery in health facilities after identifying gaps through the use of analytical tools available in DHIS2. The use of single source for analyzing immunization data facilitates detecting and spotting data quality issues as well as easier information dissemination to key stakeholders.
5. Moving Forward
HISP Tanzania continues to plan and work with the MoH and its stakeholders to roll out the integration beyond the two pilot regions. While positive results have been realized, challenges have also been noted. For example, a significant drop in coverage for immunization data in the paperless regions was observed. Assessment revealed lack of or limited technical support to the facility level users as the main obstacle. Introducing new technologies at the facility level requires continuous support ensuring the capacity and confidence the users have towards using digital tools for reporting does not wither. In addition, building a strong local team managing the platforms is necessary for the sustainability of the integration. Remote technical support of platform leads to slower adoption of local requirements something that limits continuous use of the systems. As a results, the MoH and HISP Tanzania are working on the mechanisms for establishing a strong technical team housed within a local organization to sustain the integration of EIS and DHIS2 as well as the Electronic Immunisation Register.