SCOPE:
MOH&FW aimed to conduct a high-quality Measles-Rubella mass campaign from 12 December 2020 to 31 January 2021 to vaccinate 34,061,291 children from 9 month to <10 years and to achieve > 95% coverage of target children. In this COVID19 pandemic situation, MOH&FW prepared to conduct the vaccination campaign with safe conditions, and without causing any undue harm to the health workers and the community as well. Since, the educational institutes were not opened yet, the Government decided to conduct the community campaign through routine outreach, and newly established additional EPI sites and fixed sites.
To ensure campaign quality and monitor the campaign performance and progress, UNICEF Bangladesh has provided all sorts of technical assistance to MOH&FW, including:
-
development and implementation of a web based DHIS2 system for online microplanning, planning of vaccine and logistics distribution, and daily reporting of vaccination completed.
-
development and implementation of DHIS2 android apps with features of GPS coordinates for Supervision, Household Visits and Rapid Convenience Monitoring which will work both online and offline to cover Hard to Reach and no network areas; and
-
development of public dashboard using Laravel framework to monitor campaign performance by health managers, policy makers and independent observers.
MR Campaign server MR Campaign Micro-plan forms
.

Supervision app RCM app
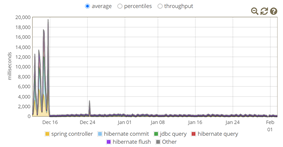
The first step was to create a separate DHIS2 instance for this campaign with latest version (2.34) to get the maximum benefit. MIS, DGHS has provided a dedicated server for optimum performance with latest Ubuntu server and PostgreSQL 12. The server was assigned 32 Core processor and 92 GB RAM. We used dhis2-tools package which is a collection of tools and utilities for installing and managing DHIS2 applications on an ubuntu server. Initially we user Apache as a proxy server but because we will be used Android app for supervision so nginx was introduced for connection load balance. To monitor server performance, we used munin and glowroot software.
Challenges
From the initial phase to the completion of the campaign UiO was supported UNICEF technical team to prepare the server and maintain it. Initial first few days we are struggling about server performance. Then DHIS2 development team and android team diagnosed the software issue and released a patch for it. After the upgrade everything ran smoothly.
A total of 403,765 organization-units for the campaign session sites (excluding parent sites) were created for reporting of micro-plan and daily vaccination and a total of 16,000 user IDs were created for using systems for supervision, HH visit and RCM app. We completed training for all the users for online microplanning, reporting, supervision, and RCM to monitor campaign performance. Bangladesh is the first and largest implementer of DHIS2-based MR campaign planning and monitoring systems using web-based DHIS2 and DHIS2 android apps. The University of Oslo (UiO) team worked closely with UNICEF, Bangladesh to support this initiative. The public dashboard which is synchronized with DHIS2 database was updated automatically daily and to facilitate policy makers and health managers to guide the campaign activities and make it a successful event.
First ever digital campaign works using DHIS2 in planning, implementing, and monitoring MR campaign 2020 of Bangladesh -
On a foggy wintry morning, exactly on the dot at 8:00 a.m. vaccinator, Sumaiya Akhter is ready to start her day at the Measles-Rubella (MR) vaccination center at East Khustia, Baliatti, Saturia Upazila in Manikganj. When vaccinators go to the center for vaccination, they have with them a complete data chart and tally sheet, making their work easier. This is the scenario of all over Bangladesh during the MR Campaign 2020. All EPI personals, Health Workers, vaccinators have their micro plan target data printed from DHIS2. As per the MR Campaign strategy, two vaccinators will work as a team in each campaign vaccination site. There is total 50,470 (approx.) teams worked to conduct the campaign.
This year the Government of Bangladesh with the support of UNICEF made breakthrough by using digital innovation. These innovations have greatly helped the health workers to identify HTR area and head count of the children eligible for immunization. For example, by making the online Micro-plan through DHIS2 (District Health Information Software), to keep track of what, when, where, which and how of the MR Campaign, the Government of Bangladesh, with the support of UNICEF, has for the first time prepared a digital Micro-plan, where all these session data are uploaded and stored in DHIS2.
The MR vaccination is every child’s right. The MR vaccination campaign aims to leave no child behind. Total target children were 34,061,291 as per the population projection and the total target was 35,337,521 as per the Micro Plan. This year the campaign has gone all digital and boasts six new digital innovation in strategy. The innovations are as follows:
• Online Micro-plan through DHIS2
Bangladesh comprises 8 divisions, 64 districts, and 12 city corporations and 111 Municipalities. EPI services in subnational rural areas rely on a system of 64 Districts, 483 Upazilas, 4,599 Unions, 13797 Wards, and 110,376 Sub-blocks within the Wards and urban immunization relies on 12 City Corporations, 111 Municipalities and 1469 wards.
Each ward is divided into eight sub-blocks namely KA 1, KA 2 until GHA 2 (according to Bengali alphabets). These sub blocks have campaign sites in turn and are divided in three campaign sites for example KA 1 has A, B, C as sites up until GHA 2- A, B, and C. Total campaign sites numbered 402,672 (Rural 331,128 and Urban 71,544) and all these sites were addressed in DHIS2 as organization units.
Three types of dataset were developed for Outreach center, Fixed center, and Hard-to-reach/High Risk centers micro plans.
All the session information was uploaded in detail, including:
- how many children are there in one center,
- which two vaccinators will conduct the session,
- which volunteers will help,
- which first line supervisor will be there to oversee the session,
- which porter will carry the vaccine
Based on the target number entered in the micro plan form, all the required numbers of MR Vials, Diluents, AD syringe, Mixing Syringe, Safety box, Vaccine carrier, and AEFI forms were populated in the system automatically. This digital Micro-plan was readied according to their campaign session dates before the start of the campaign. This enabled health managers for real time daily monitoring of coverage against target and gap, if any.
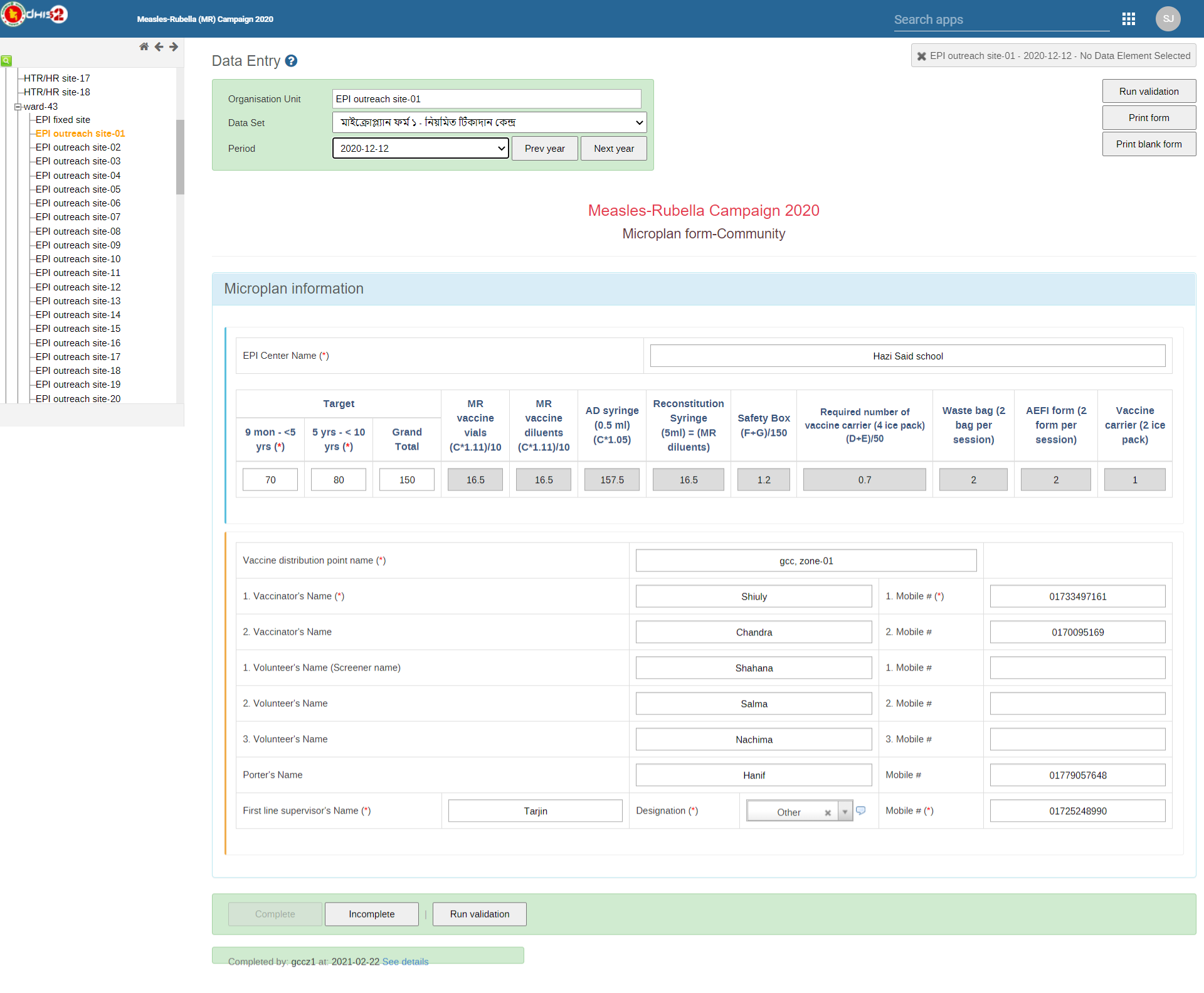
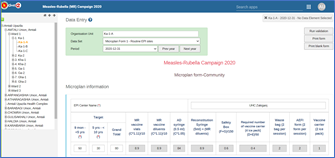
Micro plan forms
• Daily vaccine and logistics requirement and distribution plan through DHIS2
As per micro plan target, the required number of vaccine vials and syringes for each center, and logistics management plans were prepared automatically. Earlier these were done in writing, which was a tedious process. This time all Upazila, Municipality and City Corporation EPI personal prepared the daily vaccine and logistic distribution plan for each session through DHIS2 pivot table. According to this daily vaccine and logistic distribution plan the EPI supervisor distributed the required vaccine and logistics to each team during campaign.
Every morning the supply chain information of MR Campaign was easily downloaded from DHIS2 as per micro plans.
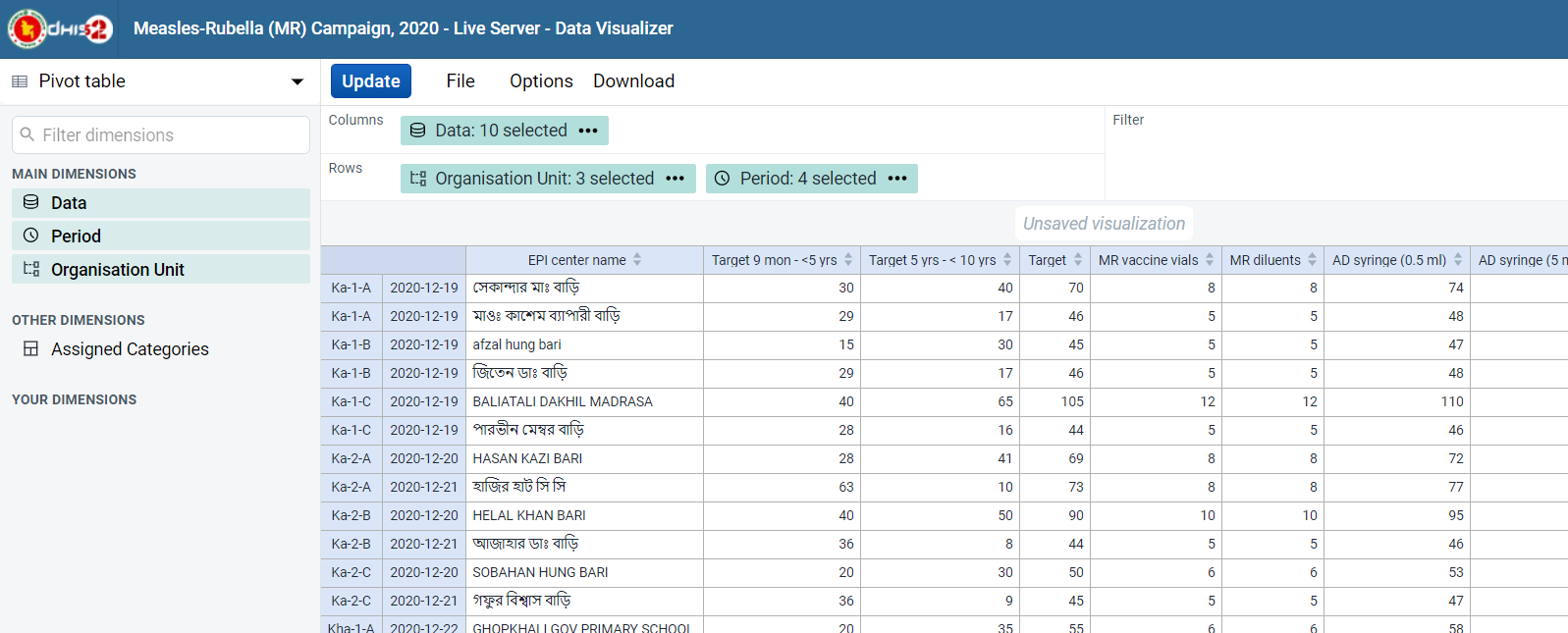
Vaccine & Logistics distribution plan
• Daily reporting through DHIS2
Schedule reporting from the required target tally form is uploaded by the Medical Technologists- Extended Programme on Immunization (MT- EPI) after the session is completed every day during the MR Campaign -
- how many children were vaccinated,
- how many vials and syringes were used, etc.
The health managers monitored the vaccine, syringes and other logistics uses and wastage from reporting format using pivot tables. Also, the Independent observers and second line supervisors monitored the campaign performance and progresses from Upazila, District, Division, and national level on daily basis.
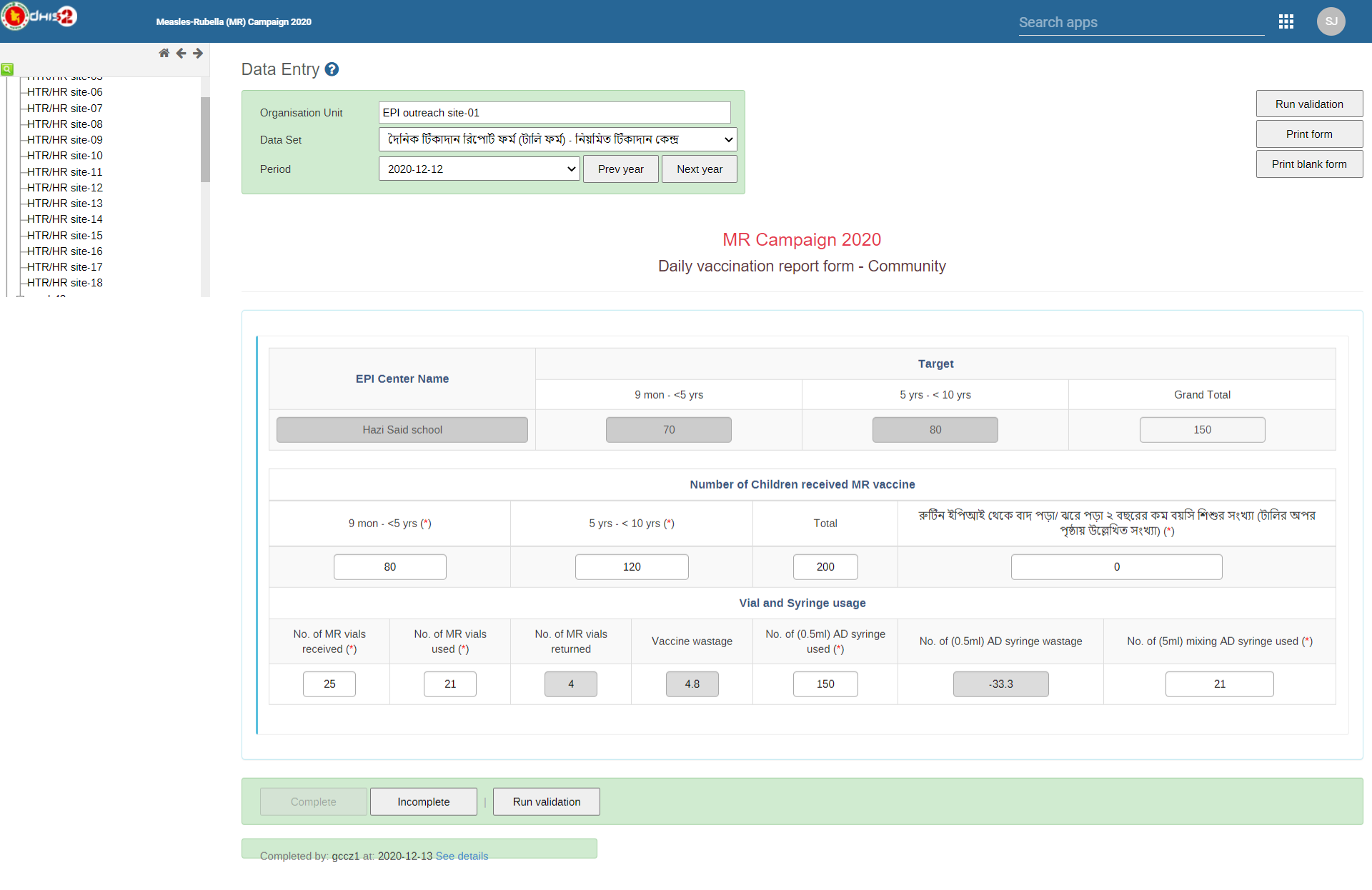
Daily vaccination form
• Supervision through android base mobile App using DHIS2 capture app
This is a field application to supervise campaign session for both first- and second-line supervisors. Earlier it was all handwritten, now through the DHIS2 application, real time data was uploaded smoothly, including geolocation and the qualitative feedbacks to monitor the campaign performance. The traditional supervision checklist transformed into the digital app using DHIS2 capture app. This helped national, divisional, district and sub-district level health managers enable real time monitoring of the campaign performance and decision making.

MR Campaign session supervision through DHIS2 app
Aminul Islam, Assistant Health Inspector (AHI) and also the first line supervisor uses his android mobile application to monitor if the vaccinators are taking the right vaccine intake, whether they are keeping the correct tally, and if anything is amiss. They upload the required data of worker attendance, session attendance, session organization, session conduction, waste management, Adverse Effect Following Immunization (AEFI) management, the cold chain maintenance, vaccine temperature control, and logistics through the android mobile application.
• Household (HH) visit by 1st line supervisor through android application
House to house visit conducted on next day by first line supervisor where campaign session was done to check and see if the vaccination data and coverage implemented and each of the target children of that area received the vaccine. All supervisors used their android mobile to conduct this house to house visit through DHIS2 android capture app “Household Visit”. All the inputs were uploaded and anyone working on the campaign can easily gain access. If any child were left out, the app shows the alert that is visible to the health manager and EPI supervisors of that catchment area so they can prepare a mop-up vaccination plan.
The health workers, while conducting the HH (house to house) survey make an entry of all the unvaccinated children who are unavailable or indisposed. For instance, there are children who are either sick or visiting grandparents and are not available for MR vaccine on the regular session day. Such children are brought under coverage through special mop-up sessions.
The UH&FPO monitored the HH visit finding through DHIS2 from his office and planned for mop-up session in the area along with the MT-EPI.


Conducting Household visit through DHIS2 app
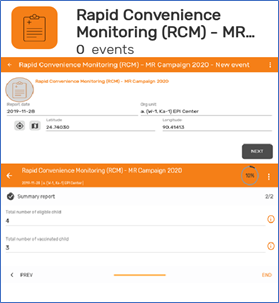
• Rapid Convenience Monitoring (RCM) by 2nd line and other supervisor of all level through android Application
Rapid convenience monitoring (RCM) has been used for years as the primary method for monitoring mass vaccination campaigns. Previously RCM was conducted as paper-based system. For MR Campaign 2020 the paper-based RCM transformed into a digital system using DHIS2 capture app, and this system was widely used by Managers, Doctors, WHO officials, UNICEF officials and other partners to monitor MR Campaign 2020 using DHIS2 android based RCM app.
Some of the inputs on sessions conducted were how many children were vaccinated, how many were male and female, etc. If a child was not vaccinated then why it did not happen, to make certain that they are included in the next mop up session. This is a manager level application with more detailed monitoring steps. Earlier these information were not collected this quickly. Now with the application everything has become easier. According to the RCM 98.1% of children were vaccinated. During the campaign corrective measures has been taken where area found RCM coverage <95%. Real time monitoring including capturing Global Positioning System coordinates through the RCM app using DHIS2 android app enabled health managers to take the decision promptly where the mop-up or additional vaccination session were required.
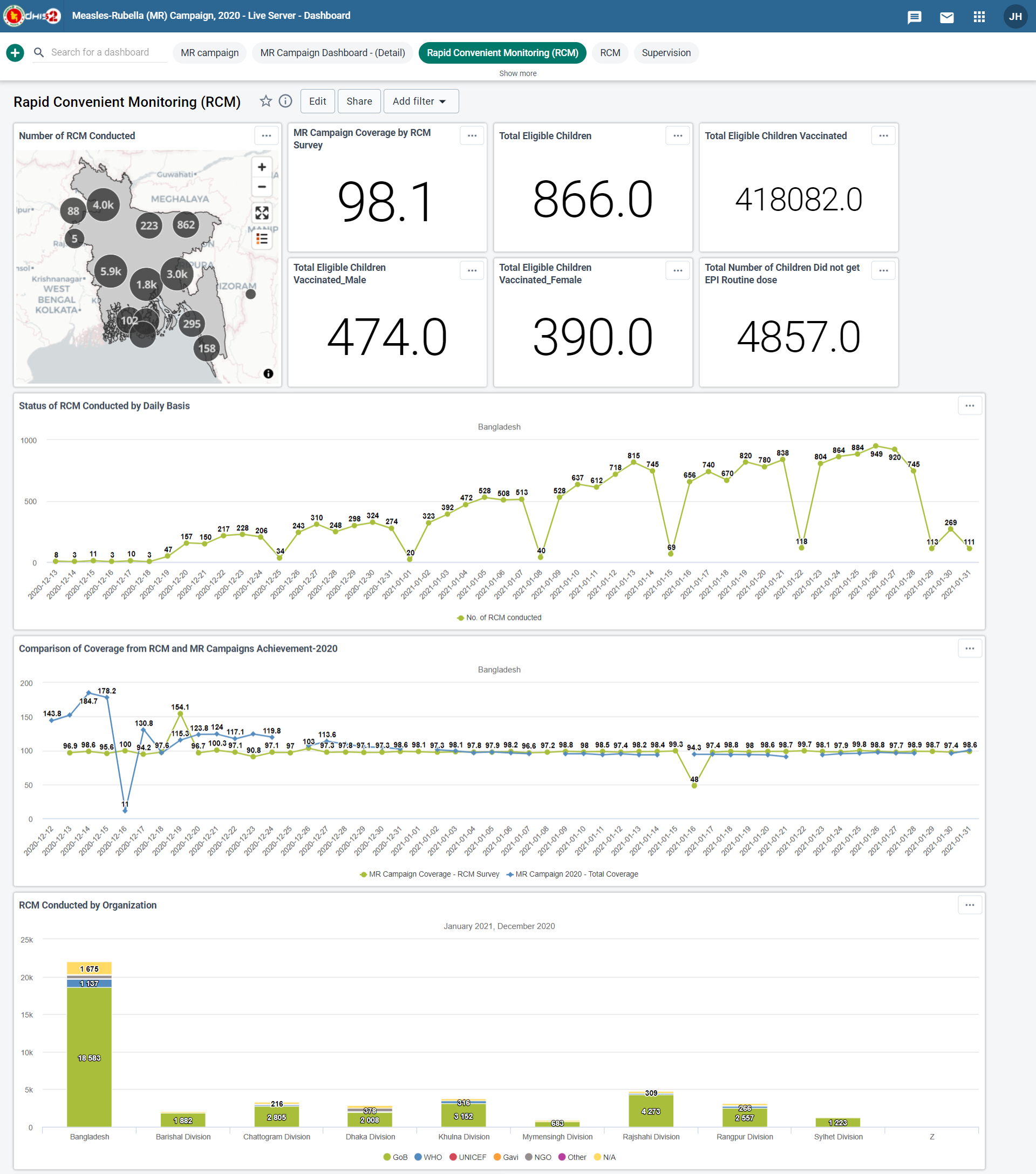
RCM Dashboard
• Campaign monitoring dashboard for all level which will allow to monitor campaign coverage up to session level along with quality aspect of the campaign. online reporting, RMC, Micro-plan, HH visits — these data were extracted through the DHIS2 API and uploaded in the external dashboard. The campaign has a systematic strategy to guarantee that each child is vaccinated.
Public Dashboard - http://103.247.238.92/mrcampaign/public/

MR Campaign public dashboard
Implementation process of these digital innovation of MR Campaign 2020 through DHIS2 –
As Bangladesh implemented the DHIS2 throughout the country since 2010 and it is the main platform for the HMIS of Bangladesh, i.e facility-based users are well efficinet in reporting at aggregated, Tracker Capture and Event Capture in DHIS2. However, the community health service providers in rural and urban were not trained enough in DHIS2. As the MR Campaign was sheduled in March 2020 then we conducted face to face training for all facility and community level users (50,470 approx.).
At the begening we conducted field-test of the MR Campaign Online Microplan, Vaccination Report, Vaccine and Logistics distribution plan, Supervision and RCM apps in both Urban and Rural area. Following that a workshop on review and finalization of these online micro plan, reporting, supervision, and RCM apps was held at the national level. After finalization of all the MR Campaign eTools in DHIS2, the National level ToT conducted for the Pool of the trainers on online microplanning, reporting, supervision, RCM apps and dashboard uses. These Pool trainner were responsible to conduct the Training at Divisional (State) and City Corporation level training. Then the Divisional and City Corporation level trainners facilitated respectively the District, Sub-district, and City Corporation Zone level training according to the training plan. It took almost 6 months from the planning, development, field testing, review, and finalization of these tools to comepletion of all user’s level training. As the MR Campaign postponed for 9 Months due to COVID-19 pandemic therefore we had to conduct refresher training through online for all users by 1 month. Training focused on reporting, analysis of data daily so that it could help them to monitor campaign performance and progress on regular basis and enhance local level descision making whenever required such as planning for mom-up campaign if any child missed in a catchment during the campaign.
The motto is to leave no child behind. The first digital MR campaign has been very effective for reaching Hard to Reach and High Risk group populations.
Comments from the end user of this digital system –
Mr. Saiful Islam, Medical Technologist EPI (MT-EPI), Saturia Upazila, Manikganj, Bangladesh -
“I have been working in this field for more than 10 years and have immunized thousands of children. However, with this year’s digital Micro-plan, our reporting, supervision, data entry and most importantly our accountability has increased multiple times. With the digital system we can get the picture of entire Bangladesh by sitting in our offices,”